Summary
What is PSA?
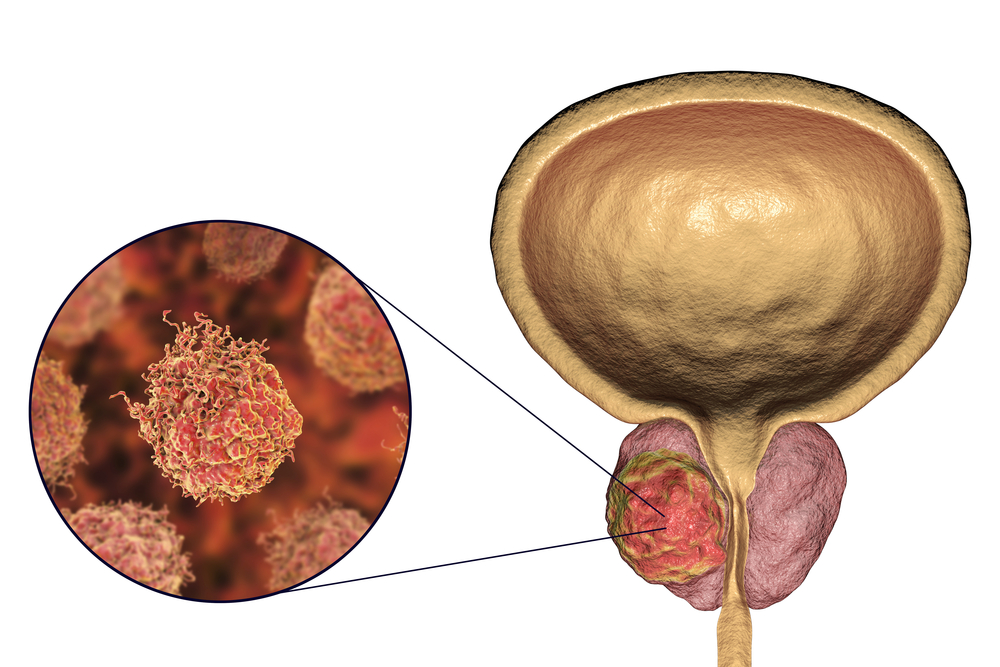
PSA is a protein made by the prostate cells. Its job is to liquefy semen. Small amounts leak into the bloodstream where it can be measured. In most prostate cancer, more PSA gets into the blood than normal.
PSA is measured to screen for prostate cancer, and to monitor the response to treatment in people who have prostate cancer. However, rises in PSA levels can be caused by many factors and are not always due to prostate cancer. The PSA test cannot specifically test for cancer and can only show if more PSA is getting into the bloodstream. By itself it cannot diagnose prostate cancer.

Two forms of PSA
PSA exists in two forms in the blood:
The most common test is the total PSA which measures the sum of both. When a doctor orders a PSA test, they are referring to a total PSA test.
Free PSA is sometimes ordered when total PSA levels are only slightly raised. The test is used to help differentiate between prostate cancer and non-cancerous conditions.
Why get tested?
Raised levels of PSA are associated with prostate cancer, but they are also seen with prostatitis (inflammation of the prostate) and benign prostatic hyperplasia (BPH) (a big or enlarged prostate). PSA levels also tend to increase naturally as men age.
BPH – benign prostatic hyperplasia
Two-thirds of men who see their doctor with high PSA levels have non-cancerous conditions. BPH is a non-cancerous swelling of the prostate that mostly occurs in older men. Because the prostate gland tends to get bigger with age, it can squeeze the urethra (the tube that drains urine out of your body) and cause problems in passing urine.
Prostatitis
This is inflammation of the prostate usually caused by an infection, most often when bacteria spill into the prostate from the urinary tract. It can be acute – it comes on suddenly for a short time - or chronic which means it is on-going. People with prostatitis often have other symptoms such as discomfort and tenderness. Prostatitis is treated with antibiotics.
Many things can cause temporary rises in PSA levels. This includes anything that disturbs the prostate such as riding a bike or motorbike, vigorous exercise, having a rectal examination, an orgasm within the past 24 hours or prostate surgery. Some medications are known to raise levels.
Since prostate cancer shares similar symptoms with many other conditions, your doctor may order other tests, such as a urine culture. If a total PSA level is raised, they may order a repeat test a few weeks later to see whether the PSA levels have returned to normal.
Should you get tested?
The likelihood of being diagnosed with prostate cancer increases with age. For Australian men the chance of being diagnosed by age 75 is 1 in 7, and by age 85 this increases to 1 in 5.
The only way to definitively diagnose prostate cancer is to take a biopsy. This is a test where a small sample of tissue from the prostate gland is collected and examined for cancer. The biopsy test is not always perfect and can miss the cancer even when it is present.
PSA testing is widely used, but experts still disagree about whether population PSA screening (testing the PSA of all men of a certain age) provides more benefit than harm. PSA can help detect prostate cancer earlier. Compared to other cancers, prostate cancer has one of the highest five-year survival rates, especially if treated early. However, it can also lead to false positive results and overdiagnosis, and treatments that cause long‑term side effects. Many men treated for prostate cancer experience ongoing side effects that impact on their quality of life.
There is a lot of conflicting advice about PSA testing. However, long-term data on PSA screening for prostate cancer shows that people who have regular PSA tests have a lower risk of death from prostate cancer compared with those who do not have regular screening. So, before getting a PSA test, talk to your doctor about the benefits and risks of having this test. Then you can decide if you wish to go ahead or not.
Prostate cancer is the most commonly diagnosed cancer in men and the second most common cause of death from cancer in Australian men, with indigenous men having a higher rate of prostate cancer mortality. The Australian Government Position Statement on PSA testing recommends offering testing from the age of 50 years to men who have been informed of the risks and benefits of PSA testing for prostate cancer.
The Urological Society of ANZ recommends that PSA testing be offered to men that have a high chance of prostate cancer, but not to all men.
Men at a high risk of prostate cancer are men who have a family history of prostate cancer, men of high-risk ethnicities (including indigenous men), and men who have genetic mutations that makes them more likely to develop prostate cancer. They do not recommend PSA testing for men who are not likely to live more than seven years. In men with limited life expectancy, the cancer is unlikely to cause symptoms or affect their health during their remaining lifetime.
Genetic testing for prostate cancer
Prostate cancer is highly heritable. It is estimated that up to 60 per cent of prostate cancer risk is caused by inherited factors. This is due to many genetic alterations, called variants, that are common in the general population. The more of these common variants a person has, the greater the risk of prostate cancer.
As well as this, some less common genetic variants can confer an even greater risk of prostate cancer. About 1–2 per cent of prostate cancers is due to genetic mutation in the BRCA1 and BRCA2 genes. Genetic testing for prostate cancer gene variants is available in genetic pathology laboratories across Australia for men with a family history of the disease. If you are interested in having this testing, you should speak with your GP about your family history and seek a referral to a familial genetic service.
Lifestyle factors also contribute to risk of prostate cancer such as diet, obesity, physical activity.
Having the test
Sample
Blood
Preparation
You may be advised to avoid ejaculation and vigorous physical activity affecting the prostate, such as bicycle riding, during the two days before the blood test. The sample should also be collected before the digital rectal exam and before (or several weeks after) a prostate biopsy.
Your results
Reading your test report
Your results will be presented along with those of your other tests on the same form. You will see separate columns or lines for each of these tests.
For men with an initial PSA level of more than 3 µg/L, your doctor will consider the need for further testing that may including an MRI scan and prostate biopsy.
A sudden increase in total PSA levels suggest prostatitis.
Some cancer cells do not produce much PSA, so it is possible to have a normal result yet have cancer. Recent studies have shown that there is still a small risk of prostate cancer, even if blood PSA levels are normal for your age.
PSA levels can vary, so your doctor may decide to repeat the test to compare your results over time.
The only definite way to confirm whether prostate cancer is present or not is by taking small samples from the prostate – so called prostate biopsies.
PSA ratio
The PSA ratio, or free-to-total PSA ratio, is used when total PSA levels are between 4.0 and 10.0 ug/L to distinguish between benign conditions and prostate cancer. The test measures the amount of free PSA versus total PSA in your blood. Free PSA is not bound to proteins. A lower ratio (below 10-15 per cent) suggests a higher chance of prostate cancer, while a higher ratio indicates benign conditions like benign prostatic hyperplasia (BPH).
Reference Intervals
Your results will be compared to reference intervals (sometimes called a normal range).
If your results are flagged as high or low this does not necessarily mean that anything is wrong. It depends on your personal situation.
Reference intervals for PSA vary between labs so you will need to go through your results with your doctor.
Follow-up tests
Prostate biopsy: If you have a result higher than the PSA recommended cut-off level, your doctor may arrange for you to have a biopsy. This is a surgical procedure that takes small pieces of tissue from different parts of the prostate. The samples are sent to the lab where they are processed and looked at under a microscope. A pathologist specialising in tissue investigates the prostate cells for cancer and sends a report to your doctor. They provide information on whether you have cancer, the type of cancer and whether or not it is aggressive.
Scans: If cancer is detected, you may need to have imaging tests such as MRI, CT or bone scans to see if the disease is contained to the prostate or if it has spread, and to help with management and treatment decisions.
More to know
You may come across the following terms:
Questions to ask your doctor
The choice of tests your doctor makes will be based on your medical history and symptoms. It is important that you tell them everything you think might help.
You play a central role in making sure your test results are accurate. Do everything you can to make sure the information you provide is correct and follow instructions closely.
Talk to your doctor about any medications you are taking. Find out if you need to fast or stop any particular foods, medications or supplements. These may affect your results. Ask:
More information
Pathology and diagnostic imaging reports can be added to your My Health Record. You and your healthcare provider can now access your results whenever and wherever needed.
Get further trustworthy health information and advice from healthdirect.
What is Pathology Tests Explained?
Pathology Tests Explained (PTEx) is a not-for profit group managed by a consortium of Australasian medical and scientific organisations.
With up-to-date, evidence-based information about pathology tests it is a leading trusted source for consumers.
Information is prepared and reviewed by practising pathologists and scientists and is entirely free of any commercial influence.